
Fertility Facts
Understanding your fertility potential and how things change over time
UNDERSTANDING YOUR FERTILITY POTENTIAL AND HOW THINGS CHANGE OVER TIME
What is an Egg Cell?
An egg cell, or ovum, is the female reproductive cell in animals and humans. It is one of the largest cells in the body, containing half of the genetic material needed for the creation of a new organism. During fertilization, an egg cell combines with a sperm cell, which carries the other half of the genetic material, forming a zygote that will develop into an embryo. In humans, the egg cell is produced in the ovaries through a process called oogenesis, which begins before birth and continues until menopause. Each egg contains a protective outer layer called the zona pellucida, which only allows a single sperm to penetrate and fertilize the egg, ensuring the correct amount of genetic material is present in the zygote.
Unlike other cells, egg cells have a large amount of cytoplasm and store nutrients to support the early stages of embryonic development after fertilization. This nutrient-rich cytoplasm helps provide energy and necessary components for the zygote as it divides and begins forming into a multicellular organism. The egg cell’s mitochondria also play a crucial role in energy production for these processes. Additionally, egg cells are unique in that they contribute all the mitochondria to the offspring, as sperm mitochondria do not typically survive. This results in mitochondrial DNA being inherited solely from the mother, making the egg cell essential not only for genetic inheritance but also for providing cellular structures and resources necessary for initial development.
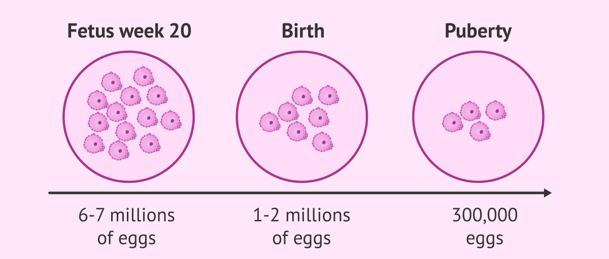
How many egg cells are found in the ovary at different times during a woman’s lifespan?
At birth, the ovaries contain approximately 1 million primordial egg cells. Each of these gg cells are genetically normal or abnormal.
After birth, there will be no further increase in egg cells.
As a woman ages, there is a predicted and constant loss of egg cells every month of her life.
The quality of the egg cells will never improve but the DNA in the egg cell can be damaged and render the egg cell to be of less quality.
At the age of 25, the number of egg cells that remain in both ovaries in total is thought to be 300,000.
The number of remaining egg cells will decline after menopause when there is no longer any egg cells left in either ovary.
How many egg cells does a woman lose each month?
Every month, 20-30 egg cells are selected to begin to develop at the beginning of the cycle. It is well-established that AMH is actually one of the factors that causes 20-30 egg cells to be selected each month from the hundreds of thousands of egg cells that the ovary contains.
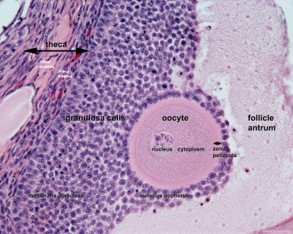
These egg cells were actually immature and are found in the primordial follicles. Immature egg cells are unable to fertilize, that is why they are called primordial. The primordial follicle is a self-contained unit found in the ovary.
After the egg is recruited or selected in the one or two follicles this month, it will move to the surface of the ovary.
FSH and LH are two hormones in the ovary that stimulate the primordial follicle and cause it to begin to mature.
This process takes 14 days until ovulation.
After ovulation, FSH and LH will actually cause the primordial follicle to be completely mature, and also assist the follicle to open up and release the matured egg contained in it. This mature egg can now be fertilized by sperm.
During the menstrual cycle, the FSH and LH will be released from the pituitary glands that will stimulate some of these 20-30 egg cells to begin to grow. The follicles that are more capable of responding to FSH and LH are the ones that will continue to grow.
In a natural cycle where no fertility medications are given, there is a limited amount of FSH and LH. So, only the best follicles will respond to these hormones. Of these follicles, there is usually one or two follicles that will continue to develop and mature and be released as matured eggs at the time of ovulation.
The largest follicle is called a dominant follicle, and that is the one that is most likely to ovulate.
When fertility medications are given, there will be much larger amounts of FSH and LH so that many more follicles will be able to respond, grow and develop until they are mature.
The other follicles will undergo a process called “ATRESIA” and they will be absorbed and disappear in the ovary.
Fertility medication contain FSH and LH. Gonal-F is FSH only while Menopur is FSH and LH.
In summary, fertility medications is the same FSH and LH found naturally in a woman’s body and in a natural menstrual cycle. These medications allow more follicles to develop and be available at the time of ovulation.
When these medications are given for IUI and IVF, most of the follicles that develop will increase in size at the same rate day-by-day.
In some cases, when we measure the number of follicles at the beginning of the cycle, we only see several. But after stimulation several days later, more follicles appear.
Several Conditions Patients should know about Fertility Medications
- Better follicles are more likely to respond to FSH and LH
- Better follicles will tend to grow at the same rate as other good follicles and be around the same size day after day during stimulation.
- Healthy follicles will usually grow 2 millimeters a day.
Example:
A follicle measures 10 millimeters on day 5 of the stimulation. One can predict that on day 6, the healthy follicle will measure 12 millimeters, day 7 is 14 millimeters, day 8 is 16 millimeters, day 9 is 18 millimeters and day 10 is 20 millimeters – at which the hCG trigger can be given.
- Using fertility medication does not cause a patient to lose eggs. These medications only act on the follicles that have been selected to grow that month. All those follicles will be gone at the end of the month where we will stimulate them and use them to get pregnant or not.
How does one determine egg count and egg quality?
- Antral follicle count – determines the number of eggs available that month.
- Anti-mullerian hormone (AMH) – blood test that determines the quality of the egg that month.
- What is Antral Follicle Count (AFC)? During the first five days of the menstrual cycle, a vaginal sonogram is done to visualize both ovaries and see how many follicles are present.
- What is Antral Follicle Count (AFC)? During the first five days of the menstrual cycle, a vaginal sonogram is done to visualize both ovaries and see how many follicles are present.
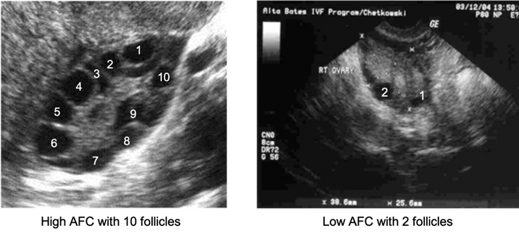
The follicle is a fluid-filled sac that contains an immature egg that is floating in the sac.
During the menstrual days, we can predict the number of eggs from each follicle of each ovary.
The AFC is very important because it tells us how many follicles our patient is producing that month, and the number of follicles we can expect to respond to stimulation whether we are given fertility drugs for IUI or IVF.
Patients with higher fertility potential are likely to have a higher AFC with at least 10 follicles.
- What is Anti-Mullerian Hormone (AMH)? AMH is a hormone produced by the gradulosa cells that make up the wall of the follicle which contains the immature egg.
AMH is a glycoprotein hormone which is a type of protein molecule that has a carbohydrate attached to it.
How does one determine egg count and egg quality?
The Major Glycoprotein Hormones Involved in the Menstrual Cycle are:
- Follicle-stimulating hormone
- Luteinizing hormone
- Thyroid-stimulating hormone
- Human chorionic gona (hCG Pregnancy Hormone)
AMH in scientific terms is a “Transforming Growth Factor” that causes the growth and differentiation of egg cells in the ovary. It is produced by the “AMH-gene” which is located in chromosome 19 in all women. Therefore, AMS helps to regulate the recruitment or growth of follicles.
AMH plays a major role in recruiting follicles each month to be available and some of these follicles will continue to develop and eventually ovulate.
Without AMH, the follicles would be in a resting state and not move to the surface of the ovary. AMH will “wake up” these resting follicles and cause 20-30 to start to frow each month.
AMH provides the energy for the follicles to start to develop.
We measure AMH through help us determine the overall egg quality and number.
AMH is a strong indication about the size of the number of follicles present referred to as the ovarian reserve.
In patients with excellent egg quality, the AMH will be as high as five (5).
In patients with poor egg quality, the AMH can be as low as one or less than one.
In patients with PCOS, we have many immature follicles compared to patients without PCOS. And because of more follicles, the level of AMH can be as high as 20.
What is the relationship between a woman’s age and her fertility potential?
There is a close relationship between fertility potential and a woman’s age often as a woman’s biologic “clock is ticking”.
When one considers the first step to do a comprehensive reliable fertility screening to determine your present ovarian reserve.
With any couple, there is no guarantee that pregnancy will be successful even if they have timed intercourse on the exact day of ovulation.
At any age, even a woman as young as 18, there is no certainty that all eggs are genetically normal.
The timing of intercourse is very important because the egg is only viable for several days and after that, it will be difficult for the sperm to penetrate and fertilize the egg. Therefore, even with perfectly timed intercourse with a healthy egg and great sperm, and no other fertility factors present – the likelihood of getting pregnant in a young couple is 25% each month.
Many doctors believed that couples should try a full year before seeing a fertility specialist. It has been my practice and strong belief in over 30 years of experience that every couple deserves a full and complete evaluation even before they try to conceive.
Why is the age of 35 important to couples trying to conceive?
After the age of 35, there is a predictable decrease in fertility potential in most couples.
A woman’s reproductive potential begins shortly after puberty at age 13 and technically continues until as long as she is ovulating and having periods until the time of menopause (which is on average of age 52).
The likelihood of pregnancy in most couples is directly related to egg quality and egg quality will decrease with age because there will be an increase number of egg cells that are not genetically perfect as well as decrease in the number of egg cells that are present.
More specifically, the likelihood of achieving pregnancy relate to age:
- Is rather constant from puberty until the age of 30
- Declines further between the age of 30 and 35
- Declines more rapidly after 35 and 40
- Declines even more significantly after the age of 40 and 44
What factors affect the egg quality on the likelihood of getting pregnant?
In patients over the age of 35, there is
- A decrease in the overall number of egg cells (lower antral follicle count)
- An increase in the number of abnormal egg cells compared to the number of egg cells.
- This will occur in a lifestyle full of pollution, stress, toxicity in water, and lost of exercise.
In patients under 20,
- Not all the eggs will be perfectly normal genetically.
- There will be a higher of egg that are normal.
- There will be more eggs to start the cycle (higher antral follicle count).
Even when an egg cell is not genetically normal ,the follicle can still continue to grow, ovulate, and be fertilized in the fallopian tube. However, most of the time, it will be less likely to fertilize, develop into an embryo, implant in the uterus and continue on as a healthy pregnancy.
Because the embryo is not genetically perfect, in most cases, the pregnancy will result in a miscarriage or a childhood birth defect. This underscores the importance of egg freezing technology to liberate woman from the reality of age-relating decline in egg number and quality and stop the biologic clock.
Egg freezing extends the opportunity to achieve pregnancy at an age of 49 by using the eggs she was able freeze and store at the age of 29.
This technology is truly “lifesaving”.
How and why does the egg quality decline in patients over 35?
After 35, the number of egg cells available will decline, causing a diminished ovarian reserve. The quality of the woman’s egg cells is a major factor in her fertility potential and the likelihood of having a child.
Eggs of high quality will have the best chance of developing a normal embryo for implanting and resulting in a successful pregnancy.
In addition to the natural decline of egg number in age, egg cells can be damaged or lost more quickly by some medical treatments which is cancer therapy or radiation.
Smoking is known to cause an earlier decline in egg quality.
Egg quality determines embryo quality, therefore, poor egg quality is often associated with chromosome abnormality embryo – known as aneuploidy.
Aneuploidy often results to miscarriage, and often the woman does not know she was pregnant. Less often, aneuploidy results to babies born with defects.
In women over the age of 35, there is an increase in number of eggs with genetic abnormalities. As eggs mature, they undergo a process of cell division called “myosis”.
The complex process of myosis must occur with a 100% accuracy. Otherwise, genetic errors will occu during the division process and the eggs will not be genetically normal.
A normal egg is genetically called a eucloid. Abnormal eggs are called aneucloid.
If the genetics of the egg cell DNA has been damaged, this can result in difficulty in having a healthy baby.
There is no blood test that directly measures the quality of the egg cell to see if it’s normal chromosomally. The only way to determine if an egg cell has a normal chromosome is to do a biopsy of an embryo formed from an egg cell, then a genetic testing.
Are there specific factors that can make the number and quality of egg cells decline at a slower rate or faster rate?
There are many studies undergoing that are trying side the factor that affect the egg cell number and slow down the ageing process.
- Avoiding or preventing medical illness such as obesity, diabetes, hypertension, anemia.
- Auto-immune disorders
- Exposure to covid virus or disease
- Recreational drugs
- Smoking and alcohol
- Sexual transmitted diseases such as chlamydia
- Age of menopause of one’s mother, grandmother, aunts and sisters.
If there is a family history of early menopause (before the age of 50) that history should be an important consideration.
Even patients have their own individual genetic likelihood of rapid or slow decline in number and egg quality. This probably can be more rapid if there are environmental factors such as toxicity, medical conditions, or illnesses. Even patients who are meticulous with their health, they may be able to slow down the loss of egg cells but not forever.
AMH level is still extremely important to help answer this question to patients.
Can fertility treatments make you more likely to get pregnant even after the age of 35?
Fertility treatment can be successful in increasing in odds of getting pregnant but fertility treatment cannot overcome completely the problem of decreased egg numbers and increased percentage of egg that are not genetically perfect.
Many studies have shown that the expected decrease in fertility potential, both in egg number and egg quality, can affect the outcome of different treatments that we offer our patients.
- Fertility medications such as Clomid, Letrozole, Gonal-F, Menopur – are greatly helpful to increase the number of egg cells that can be recruited to grow in a certain cycle. But fertility medication has a very limited effect on egg quality with a problem in perfect genetics.
- Intrauterine Insemination (IUI) is an excellent method to help couples achieve pregnancy. By concentrating the sperm sample into one to two drops and placing the drops carefully into the uterus, enters the fallopian tube to meet up with the egg cell. However, if the egg cell quality is inadequate, even with IUI, the chances for success are less.
- IVF – using fertility medication, multiple eggs can be stimulated and retrieved from the ovary and place into a petri dish. With IVF, we can inject a sperm cell into the egg and create an embryo that is later transferred to the uterus.
Theoretically, this should be a guaranteed pregnancy because the embryo is in the uterus and all it has to do is implant and it continues to grow. If unfortunately, the egg quality is poor, there will be less chance of having a healthy embryo so the IVF success rate will be less than expected for women of her age group.
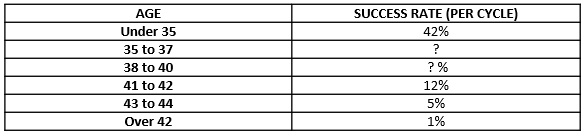
Success Rate with IVF for Women of Different Age Groups
UNDERSTANDING YOUR FERTILITY POTENTIAL AND HOW THINGS CHANGE OVER TIME
What is an Egg Cell?
An egg cell, or ovum, is the female reproductive cell in animals and humans. It is one of the largest cells in the body, containing half of the genetic material needed for the creation of a new organism. During fertilization, an egg cell combines with a sperm cell, which carries the other half of the genetic material, forming a zygote that will develop into an embryo. In humans, the egg cell is produced in the ovaries through a process called oogenesis, which begins before birth and continues until menopause. Each egg contains a protective outer layer called the zona pellucida, which only allows a single sperm to penetrate and fertilize the egg, ensuring the correct amount of genetic material is present in the zygote.
Unlike other cells, egg cells have a large amount of cytoplasm and store nutrients to support the early stages of embryonic development after fertilization. This nutrient-rich cytoplasm helps provide energy and necessary components for the zygote as it divides and begins forming into a multicellular organism. The egg cell’s mitochondria also play a crucial role in energy production for these processes. Additionally, egg cells are unique in that they contribute all the mitochondria to the offspring, as sperm mitochondria do not typically survive. This results in mitochondrial DNA being inherited solely from the mother, making the egg cell essential not only for genetic inheritance but also for providing cellular structures and resources necessary for initial development.
How many egg cells are found in the ovary at different times during a woman’s lifespan?
At birth, the ovaries contain approximately 1 million primordial egg cells. Each of these gg cells are genetically normal or abnormal.
After birth, there will be no further increase in egg cells.
As a woman ages, there is a predicted and constant loss of egg cells every month of her life.
The quality of the egg cells will never improve but the DNA in the egg cell can be damaged and render the egg cell to be of less quality.
At the age of 25, the number of egg cells that remain in both ovaries in total is thought to be 300,000.
The number of remaining egg cells will decline after menopause when there is no longer any egg cells left in either ovary.
How many egg cells does a woman lose each month?
Every month, 20-30 egg cells are selected to begin to develop at the beginning of the cycle. It is well-established that AMH is actually one of the factors that causes 20-30 egg cells to be selected each month from the hundreds of thousands of egg cells that the ovary contains.
These egg cells were actually immature and are found in the primordial follicles. Immature egg cells are unable to fertilize, that is why they are called primordial. The primordial follicle is a self-contained unit found in the ovary.
After the egg is recruited or selected in the one or two follicles this month, it will move to the surface of the ovary.
FSH and LH are two hormones in the ovary that stimulate the primordial follicle and cause it to begin to mature.
This process takes 14 days until ovulation.
After ovulation, FSH and LH will actually cause the primordial follicle to be completely mature, and also assist the follicle to open up and release the matured egg contained in it. This mature egg can now be fertilized by sperm.
During the menstrual cycle, the FSH and LH will be released from the pituitary glands that will stimulate some of these 20-30 egg cells to begin to grow. The follicles that are more capable of responding to FSH and LH are the ones that will continue to grow.
In a natural cycle where no fertility medications are given, there is a limited amount of FSH and LH. So, only the best follicles will respond to these hormones. Of these follicles, there is usually one or two follicles that will continue to develop and mature and be released as matured eggs at the time of ovulation.
The largest follicle is called a dominant follicle, and that is the one that is most likely to ovulate.
When fertility medications are given, there will be much larger amounts of FSH and LH so that many more follicles will be able to respond, grow and develop until they are mature.
The other follicles will undergo a process called “ATRESIA” and they will be absorbed and disappear in the ovary.
Fertility medication contain FSH and LH. Gonal-F is FSH only while Menopur is FSH and LH.
In summary, fertility medications is the same FSH and LH found naturally in a woman’s body and in a natural menstrual cycle. These medications allow more follicles to develop and be available at the time of ovulation.
When these medications are given for IUI and IVF, most of the follicles that develop will increase in size at the same rate day-by-day.
In some cases, when we measure the number of follicles at the beginning of the cycle, we only see several. But after stimulation several days later, more follicles appear.
Several Conditions Patients should know about Fertility Medications
- Better follicles are more likely to respond to FSH and LH
- Better follicles will tend to grow at the same rate as other good follicles and be around the same size day after day during stimulation.
- Healthy follicles will usually grow 2 millimeters a day.
Example:
A follicle measures 10 millimeters on day 5 of the stimulation. One can predict that on day 6, the healthy follicle will measure 12 millimeters, day 7 is 14 millimeters, day 8 is 16 millimeters, day 9 is 18 millimeters and day 10 is 20 millimeters – at which the hCG trigger can be given.
- Using fertility medication does not cause a patient to lose eggs. These medications only act on the follicles that have been selected to grow that month. All those follicles will be gone at the end of the month where we will stimulate them and use them to get pregnant or not.
How does one determine egg count and egg quality?
- Antral follicle count – determines the number of eggs available that month.
- Anti-mullerian hormone (AMH) – blood test that determines the quality of the egg that month.
- What is Antral Follicle Count (AFC)? During the first five days of the menstrual cycle, a vaginal sonogram is done to visualize both ovaries and see how many follicles are present.
- What is Antral Follicle Count (AFC)? During the first five days of the menstrual cycle, a vaginal sonogram is done to visualize both ovaries and see how many follicles are present.
The follicle is a fluid-filled sac that contains an immature egg that is floating in the sac.
During the menstrual days, we can predict the number of eggs from each follicle of each ovary.
The AFC is very important because it tells us how many follicles our patient is producing that month, and the number of follicles we can expect to respond to stimulation whether we are given fertility drugs for IUI or IVF.
Patients with higher fertility potential are likely to have a higher AFC with at least 10 follicles.
- What is Anti-Mullerian Hormone (AMH)? AMH is a hormone produced by the gradulosa cells that make up the wall of the follicle which contains the immature egg.
AMH is a glycoprotein hormone which is a type of protein molecule that has a carbohydrate attached to it.
How does one determine egg count and egg quality?
The Major Glycoprotein Hormones Involved in the Menstrual Cycle are:
- Follicle-stimulating hormone
- Luteinizing hormone
- Thyroid-stimulating hormone
- Human chorionic gona (hCG Pregnancy Hormone)
AMH in scientific terms is a “Transforming Growth Factor” that causes the growth and differentiation of egg cells in the ovary. It is produced by the “AMH-gene” which is located in chromosome 19 in all women. Therefore, AMS helps to regulate the recruitment or growth of follicles.
AMH plays a major role in recruiting follicles each month to be available and some of these follicles will continue to develop and eventually ovulate.
Without AMH, the follicles would be in a resting state and not move to the surface of the ovary. AMH will “wake up” these resting follicles and cause 20-30 to start to frow each month.
AMH provides the energy for the follicles to start to develop.
We measure AMH through help us determine the overall egg quality and number.
AMH is a strong indication about the size of the number of follicles present referred to as the ovarian reserve.
In patients with excellent egg quality, the AMH will be as high as five (5).
In patients with poor egg quality, the AMH can be as low as one or less than one.
In patients with PCOS, we have many immature follicles compared to patients without PCOS. And because of more follicles, the level of AMH can be as high as 20.
What is the relationship between a woman’s age and her fertility potential?
There is a close relationship between fertility potential and a woman’s age often as a woman’s biologic “clock is ticking”.
When one considers the first step to do a comprehensive reliable fertility screening to determine your present ovarian reserve.
With any couple, there is no guarantee that pregnancy will be successful even if they have timed intercourse on the exact day of ovulation.
At any age, even a woman as young as 18, there is no certainty that all eggs are genetically normal.
The timing of intercourse is very important because the egg is only viable for several days and after that, it will be difficult for the sperm to penetrate and fertilize the egg. Therefore, even with perfectly timed intercourse with a healthy egg and great sperm, and no other fertility factors present – the likelihood of getting pregnant in a young couple is 25% each month.
Many doctors believed that couples should try a full year before seeing a fertility specialist. It has been my practice and strong belief in over 30 years of experience that every couple deserves a full and complete evaluation even before they try to conceive.
Why is the age of 35 important to couples trying to conceive?
After the age of 35, there is a predictable decrease in fertility potential in most couples.
A woman’s reproductive potential begins shortly after puberty at age 13 and technically continues until as long as she is ovulating and having periods until the time of menopause (which is on average of age 52).
The likelihood of pregnancy in most couples is directly related to egg quality and egg quality will decrease with age because there will be an increase number of egg cells that are not genetically perfect as well as decrease in the number of egg cells that are present.
More specifically, the likelihood of achieving pregnancy relate to age:
- Is rather constant from puberty until the age of 30
- Declines further between the age of 30 and 35
- Declines more rapidly after 35 and 40
- Declines even more significantly after the age of 40 and 44
What factors affect the egg quality on the likelihood of getting pregnant?
In patients over the age of 35, there is
- A decrease in the overall number of egg cells (lower antral follicle count)
- An increase in the number of abnormal egg cells compared to the number of egg cells.
- This will occur in a lifestyle full of pollution, stress, toxicity in water, and lost of exercise.
In patients under 20,
- Not all the eggs will be perfectly normal genetically.
- There will be a higher of egg that are normal.
- There will be more eggs to start the cycle (higher antral follicle count).
Even when an egg cell is not genetically normal ,the follicle can still continue to grow, ovulate, and be fertilized in the fallopian tube. However, most of the time, it will be less likely to fertilize, develop into an embryo, implant in the uterus and continue on as a healthy pregnancy.
Because the embryo is not genetically perfect, in most cases, the pregnancy will result in a miscarriage or a childhood birth defect. This underscores the importance of egg freezing technology to liberate woman from the reality of age-relating decline in egg number and quality and stop the biologic clock.
Egg freezing extends the opportunity to achieve pregnancy at an age of 49 by using the eggs she was able freeze and store at the age of 29.
This technology is truly “lifesaving”.
How and why does the egg quality decline in patients over 35?
After 35, the number of egg cells available will decline, causing a diminished ovarian reserve. The quality of the woman’s egg cells is a major factor in her fertility potential and the likelihood of having a child.
Eggs of high quality will have the best chance of developing a normal embryo for implanting and resulting in a successful pregnancy.
In addition to the natural decline of egg number in age, egg cells can be damaged or lost more quickly by some medical treatments which is cancer therapy or radiation.
Smoking is known to cause an earlier decline in egg quality.
Egg quality determines embryo quality, therefore, poor egg quality is often associated with chromosome abnormality embryo – known as aneuploidy.
Aneuploidy often results to miscarriage, and often the woman does not know she was pregnant. Less often, aneuploidy results to babies born with defects.
In women over the age of 35, there is an increase in number of eggs with genetic abnormalities. As eggs mature, they undergo a process of cell division called “myosis”.
The complex process of myosis must occur with a 100% accuracy. Otherwise, genetic errors will occu during the division process and the eggs will not be genetically normal.
A normal egg is genetically called a eucloid. Abnormal eggs are called aneucloid.
If the genetics of the egg cell DNA has been damaged, this can result in difficulty in having a healthy baby.
There is no blood test that directly measures the quality of the egg cell to see if it’s normal chromosomally. The only way to determine if an egg cell has a normal chromosome is to do a biopsy of an embryo formed from an egg cell, then a genetic testing.
Are there specific factors that can make the number and quality of egg cells decline at a slower rate or faster rate?
There are many studies undergoing that are trying side the factor that affect the egg cell number and slow down the ageing process.
- Avoiding or preventing medical illness such as obesity, diabetes, hypertension, anemia.
- Auto-immune disorders
- Exposure to covid virus or disease
- Recreational drugs
- Smoking and alcohol
- Sexual transmitted diseases such as chlamydia
- Age of menopause of one’s mother, grandmother, aunts and sisters.
If there is a family history of early menopause (before the age of 50) that history should be an important consideration.
Even patients have their own individual genetic likelihood of rapid or slow decline in number and egg quality. This probably can be more rapid if there are environmental factors such as toxicity, medical conditions, or illnesses. Even patients who are meticulous with their health, they may be able to slow down the loss of egg cells but not forever.
AMH level is still extremely important to help answer this question to patients.
Can fertility treatments make you more likely to get pregnant even after the age of 35?
Fertility treatment can be successful in increasing in odds of getting pregnant but fertility treatment cannot overcome completely the problem of decreased egg numbers and increased percentage of egg that are not genetically perfect.
Many studies have shown that the expected decrease in fertility potential, both in egg number and egg quality, can affect the outcome of different treatments that we offer our patients.
- Fertility medications such as Clomid, Letrozole, Gonal-F, Menopur – are greatly helpful to increase the number of egg cells that can be recruited to grow in a certain cycle. But fertility medication has a very limited effect on egg quality with a problem in perfect genetics.
- Intrauterine Insemination (IUI) is an excellent method to help couples achieve pregnancy. By concentrating the sperm sample into one to two drops and placing the drops carefully into the uterus, enters the fallopian tube to meet up with the egg cell. However, if the egg cell quality is inadequate, even with IUI, the chances for success are less.
- IVF – using fertility medication, multiple eggs can be stimulated and retrieved from the ovary and place into a petri dish. With IVF, we can inject a sperm cell into the egg and create an embryo that is later transferred to the uterus.
Theoretically, this should be a guaranteed pregnancy because the embryo is in the uterus and all it has to do is implant and it continues to grow. If unfortunately, the egg quality is poor, there will be less chance of having a healthy embryo so the IVF success rate will be less than expected for women of her age group.
Success Rate with IVF for Women of Different Age Groups
